
I will be writing general interest and medical scientific notes under #DocChain tag and community every 15 or 20 days. If it brings value to someone or you want to share, I will be very happy.
Let's hope that everything contributes to the development of #Nostr
Featured on Habla (nprofile…varq) and Highlighter (nprofile…e69h) on the first note I'm going to try to debunk all the myths you have about HIV. I'll be happy to answer any questions you may have.
Derek Ross (nprofile…jrmw) you can read it while enjoying your outdoor wedding today 😜
Introduction
The human immunodeficiency virus (HIV) began as a pandemic in the 1980s. In its early days, it was seen as a certain death sentence, a taboo associated with marginalized groups, and it highlighted the failures of poverty in accessing healthcare. Gradually, the struggle for life and the suffering of those who are no longer with us, including both famous and anonymous individuals, became visible.
Today, 40 years later, HIV is presented as a chronic disease with effective treatment. Patients living with HIV who receive appropriate treatment have no detectable virus in their circulating blood, enjoy a good quality of life, and are more concerned about other aspects of their health during medical consultations, almost forgetting their condition. For these patients, daily treatment is the cure, similar to someone taking a pill every day for high blood pressure or diabetes.
The Global Impact
HIV is a lentivirus, a subgroup of retroviruses composed of RNA. The natural history of HIV infection involves an attack on the immune system, particularly targeting CD4 cells, where chronic deterioration can lead to the acquisition of infectious and oncological diseases that may be fatal over the years, resulting in acquired immunodeficiency syndrome (AIDS).
Interestingly, there is a small group of people known as “elite controllers” who manage to control HIV infection without treatment and remain healthy for much of their lives, despite having a hidden deep viral reservoir. The primary modes of transmission are sexual, followed by blood and vertical transmission from mother to child, with the first mode predominating today.
Today, in the downward trend of the HIV epidemic, it is estimated that 39 million people are living with HIV worldwide. Depending on the region, nearly half of this population belongs to at-risk groups, such as men who have sex with men (MSM), transgender individuals, sex workers, and people who inject drugs. These vulnerable groups are especially important for prevention efforts. However, little is done for prevention in the general population, which sometimes represents the other half of the cake of people living with HIV (PLWH).
Breaking the Dogma: The Concept of Undetectable = Untransmittable (U=U)
The introduction of highly effective antiretroviral therapy (HAART) in 1994 broke the curve of the HIV epidemic. The introduction of new medications with fewer side effects and greater effectiveness in controlling the virus has been crucial. In 2007, the launch of Raltegravir as the first viral integrase inhibitor marked a milestone in current treatments, allowing patients to effectively control the virus within 3 to 6 months.
The positive impact of these treatments led health organizations to launch the concept of undetectable = untransmittable (U=U) to impact the general population and at-risk groups, updating the dogma and eradicating stigma: a patient living with HIV who maintains an undetectable viral load in their blood through treatment will not transmit HIV sexually.
Although this concept has transformed the social dynamics and stigma surrounding the disease, adherence to treatment must be complete to achieve this new paradigm.
Prophylaxis as a Method to Prevent HIV in Healthy Populations
The correct use of condoms has been the cornerstone of HIV prevention and other sexually transmitted infections over the years. However, it is not the only tool available today and can be complemented for comprehensive sexual health.
Pre-exposure prophylaxis (PrEP) is a novel strategy that involves administering antiretroviral medication to vulnerable groups before they are exposed to HIV (MSM, transgender individuals, sex workers, people who inject drugs). It involves taking medication daily, effectively reducing the risk of contracting HIV and providing protection to these groups. It is similar to taking a contraceptive pill daily. It has had a very positive impact on protecting these populations. In the Americas, it has been successfully implemented in the United States, Mexico, Peru, and Brazil. Other countries, although with some delay, are now implementing this strategy.
Post-exposure prophylaxis (PEP), on the other hand, is a strategy that involves administering antiretroviral treatment after a potential exposure to HIV. If the treatment is administered within the first 72 hours and maintained for 4 weeks, the chances of contracting HIV decrease substantially.
Both strategies have been remarkably successful in preventing HIV in at-risk populations and healthy populations, although their dissemination and awareness remain limited.
https://image.nostr.build/08682bf763ade56741d8e4c8c6d870cb8d71ab7d72c605b9aa805af2234348ff.jpg
The New Horizon: Long-Acting Antiretrovirals, HIV Vaccines, and Promising Therapies
The introduction of viral integrase inhibitors and new nucleoside analogs in the last 15 years has allowed for the availability of safe drugs with minimal side effects in the treatment of HIV, many of which are included in a single pill regimen per day. However, the pharmaceutical industry continues to diversify the offerings in a healthy manner.
Cabotegravir is a new long-acting integrase inhibitor that is administered via injection. Combined with Rilpivirine, it has proven to be effective and safe in the treatment of HIV, with injections every 2 months. This has revolutionized treatment for people who are tired of taking pills daily, as well as in PrEP, where effective prevention against HIV can be achieved with injections every 2 months for at-risk groups.
Additionally, subdermal implants of Islatravir, a new long-acting nucleoside analog, are being tested as a PrEP strategy. Similar to monthly hormonal contraceptive injections or hormonal contraceptive implants, this strategy has proven effective in at-risk groups.
Regarding the HIV vaccine, we have been developing it for over two decades, with advances and setbacks. While vaccines have shown promising results in terms of safety and antibody generation, we still need to await conclusive phase III results demonstrating their effectiveness in at-risk groups and the general population.
The Eradication of HIV and Patients Cured Without Treatment
While current treatment allows for the elimination of HIV from the bloodstream and sexual transmission, there remains a reservoir in some deep immune cells that have been infected by the retrovirus, which contain latent HIV DNA and have the potential to reactivate if daily treatment is interrupted.
However, there are patients who have managed to eliminate HIV from their bodies, including these deep cells, and HIV is undetectable upon discontinuation of treatment. These cases are very rare, with only 7 to 8 individuals being the subject of intensive scientific study. Among them are the “Berlin patient” of Germany and “City of Hope patient” from Argentina. Some of these cases involved patients under effective HIV treatment who underwent suppressive chemotherapy for bone marrow transplants and managed to eliminate these deep cells with latent HIV DNA.
Unfortunately, this treatment is not scalable for the entire HIV-positive population, both due to its cost and potential side effects. However, “Shock and Kill” strategies have been proposed, aiming to use monoclonal antibodies to activate these latent cells during HIV treatment, exposing them to antiretroviral medication for elimination, thereby eradicating these small reservoirs of HIV.
WHO Goals
The World Health Organization (WHO) has established clear objectives that are constantly updated to achieve the eradication of HIV in the population.
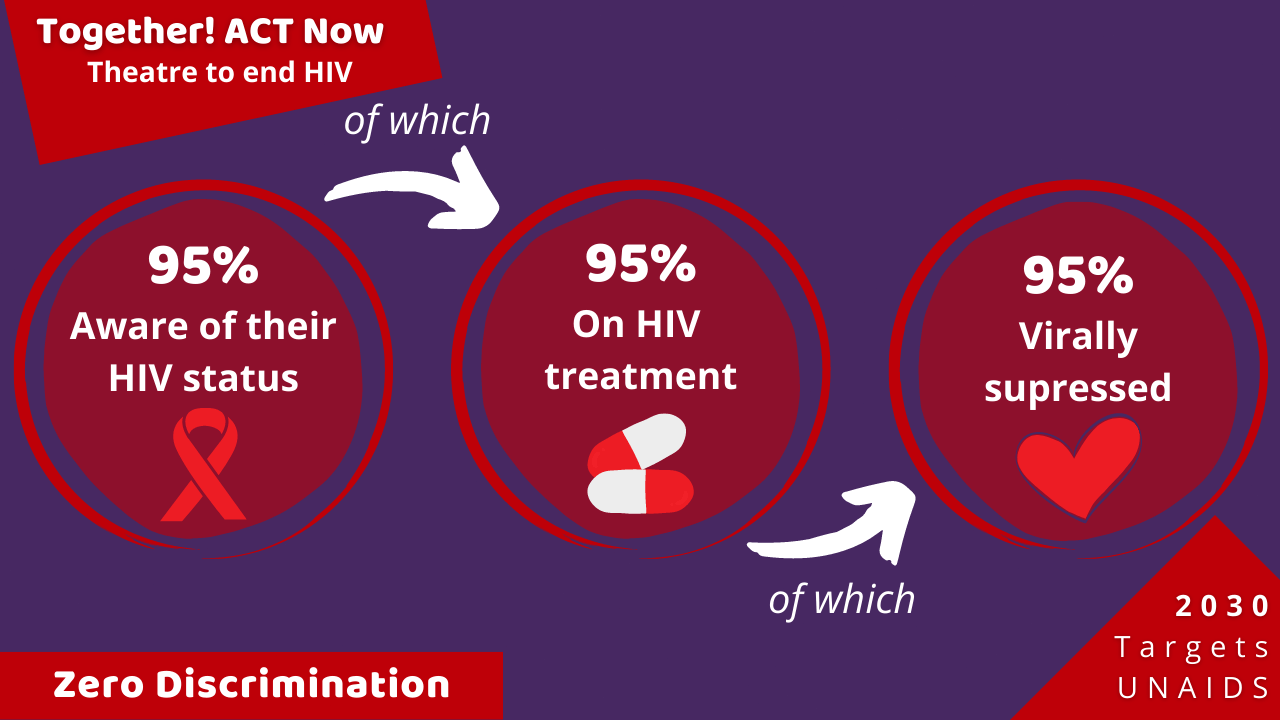
The updated goals of the WHO propose that, to end the HIV epidemic, three objectives must be met by the year 2025-2030:
- 95% of people living with HIV must be diagnosed through testing.
- 95% of diagnosed individuals must be on highly effective antiretroviral therapy (HAART).
- 95% of those on HAART must have an undetectable viral load in their blood.
Developing and underdeveloped countries currently have an effectiveness rate for these strategies that disagree significantly.
https://image.nostr.build/ac6693df57aaca6dac0b06b5db9eb1a2757e7c08511edb0f11617e12653d3db5.png
Key Takeaways
- HIV has a cure, and the cure is permanent treatment.
- Treatment for HIV is free and accessible to the population, as it is a public health impact disease.
- A person living with HIV who receives appropriate treatment will not transmit the virus sexually, will enjoy a full life without the disease, and can have children without HIV.
- In the event of a potential HIV exposure (such as unprotected sexual contact with an infrequent partner), you can go to a hospital within the first 72 hours to receive treatment that will prevent HIV infection.
- Just as we witnessed the eradication of smallpox from the face of the earth in 1978 due to scientific advances, we will live to see the eradication of HIV.
Autor
Kamo Weasel - MD Infectious Diseases - MD Internal Medicine - #DocChain Community npub1jdvvva54m8nchh3t708pav99qk24x6rkx2sh0e7jthh0l8efzt7q9y7jlj
Resources
Bibliography
- The natural history of HIV infection. DOI: 10.1097/COH.0b013e328361fa66
- Changing Knowledge and Attitudes Towards HIV Treatment-as-Prevention and “Undetectable = Untransmittable”: A Systematic Review. DOI: 10.1007/s10461-021-03296-8
- Challenges of HIV diagnosis and management in the context of pre-exposure prophylaxis (PrEP), post-exposure prophylaxis (PEP), test and start and acute HIV infection: a scoping review. DOI: 10.1002/jia2.25419
- Long-acting cabotegravir and rilpivirine dosed every 2 months in adults with HIV-1 infection (ATLAS-2M), 48-week results: a randomised, multicentre, open-label, phase 3b, non-inferiority study. DOI: 10.1016/S0140-6736(20)32666-0
- Efficacy and safety of long-acting cabotegravir compared with daily oral tenofovir disoproxil fumarate plus emtricitabine to prevent HIV infection in cisgender men and transgender women who have sex with men 1 year after study unblinding: a secondary analysis of the phase 2b and 3 HPTN 083 randomised controlled trial. DOI: 10.1016/S2352-3018(23)00261-8
- Safety and immunogenicity of a subtype C ALVAC-HIV (vCP2438) vaccine prime plus bivalent subtype C gp120 vaccine boost adjuvanted with MF59 or alum in healthy adults without HIV (HVTN 107): A phase 1/2a randomized trial. DOI: 10.1371/journal.pmed.1004360
- Shock and kill within the CNS: A promising HIV eradication approach?. DOI: 10.1002/JLB.5VMR0122-046RRR
{kind=link}
{kind=link}